A detailed study of the course, branching pattern and variations of the internal iliac artery and its branches.
ABSTRACT:
The blood supply of a region is determined by functional considerations, such that structures participating in a common activity tend to receive their blood supply from the same arterial source. Though the internal iliac artery (IIA) plays a critical role in the blood supply to the pelvic organs and cavity, and the gluteal region there is a paucity of descriptions of the origin, course, and dimensions of the IIA or its branches. The aim of the study was to present a detailed account of the pattern of blood supply of the IIA and its branches based on a cadaveric study on pelvic halves of 15 male and 16 female embalmed cadavers belonging an Indian population,.
INTRODUCTION:
The blood supply of a region is determined by functional considerations, such that structures participating in a common activity tend to receive their blood supply from the same arterial source. This inevitably make simultaneous demands on a limited blood supply, and hence, the pattern of arterial branching is fundamental to the understanding of the efficiency of blood supply to a region. While detailed reports exist of the hemodynamics of the certain arteries such as the coronary arteries, and aortic segments none exist of the internal iliac artery (IIA) or its branches despite its critical role in the blood supply to the pelvic cavity and gluteal region.
ANATOMY OF THE INTERNAL ILIAC ARTERY
The IIA, also known as the hypogastric artery, is one of the terminal branches of the common iliac artery (CIA), the other terminal branch being the external iliac artery (EIA). While the EIA supplies the lower extremity, the IIA supplies the pelvic viscera, perineum, pelvic wall and gluteal region.
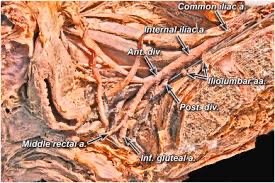
The IIA has been described in literature to typically originate from the CIA at the level of the intervertebral disc, usually between L5 and S1 vertebrae (Talalwah and Soames, 2014). It descends posteromedially into the lesser pelvis, medial to the internal iliac vein and obturator nerve, and lateral to the peritoneum which separates it from the terminal ileum on the right side and the sigmoid colon on the left side. The internal iliac vein and the lumbosacral nerve trunk are located between the IIA and the sacro-iliac joint, and the ureter is located at the medial aspect of IIA. The IIA then descends posteriorly within the pelvic cavity to divide into posterior and anterior divisions at the upper margin of the greater sciatic foramen. The anterior division continues towards the ischial spine, while the posterior division passes posteriorly towards the greater sciatic foramen to exit the pelvic cavity. The anterior trunk has both parietal and visceral branches, while the posterior trunk only has parietal branches. A detailed description of the distribution of branches of the IIA is beyond the scope of this article and only the salient features of each individual branch is discussed.
AIM OF STUDY:
A patchwork of information exists regarding details of the vascular anatomy of the IIA and its branches. Hence, this study aims to provide a detailed account of the level and mode of origin and termination, length and mean external diameter of the IIA and its branches in an Indian population. It also aims to compare the results of this study with previously reported anatomical, physiological surgical, and radiological studies on the IIA and its branches.
Internal iliac artery (IIA)
In all specimens, on both sides, the IIA originated as a terminal branch of CIA and was located anterior to sacroiliac joint. The most common level of its origin was at the upper margin of the L5 vertebra (51.61%) and the next common level was between L5 and S1 vertebra (25.81%). In a lesser number of specimens, the IIA originated between L4 and L5 vertebra (16.13%), and at the S1 vertebrae (6.45%) (Table 1). The vertebral levels of origin of the IIA on both sides of individual cadavers were identical. There were no significant differences in the levels of origin of the IIA between both sides of individual cadavers (p>0.05), or among male and female cadavers (p>0.05).
The IIA had a normal course in all the specimens and could be recognized as it descended posteromedially into the lesser pelvis, where it divided into posterior and anterior divisions. In all the cadavers the IIA was located medial to the internal iliac vein and obturator nerve, and lateral to the ureter. The anterior division continued towards the ischial spine, while the posterior division exited the pelvic cavity through the greater sciatic foramen.
Branching patterns of the anterior division of internal iliac artery
Obliterated umbilical artery
In all the cadavers, the distal part of the ULA was obliterated to form the corresponding medial umbilical ligament, which could be recognized as a cord like structure extending anteroinferiorly between the urinary bladder and the lateral wall of the pelvis. The proximal part of the ULA remained patent as the SV in all the cadavers. The dimension of the medial umbilical ligament was not recorded in any of the specimens.
Superior vesical artery
The SV originated from the root of the umbilical artery in both male and female cadavers, and it coursed medially and inferiorly in all the cadavers. Multiple branches to the superior surface of the urinary bladder and ureter could be recognized, and extensive anastomoses could also be observed with the branches of the IV in males. The origin and distribution of the SV was bilaterally identical in all the cadavers. No anatomical variations were observed in its origin, course and distribution in both male and female cadavers.
Inferior vesical artery
The IV observed only in male cadavers, and hence the observations are based on 30 male pelvic halves. In all the cadavers the IV originated from the anterior division of the IIA, descended infero-medially and provided branches to urinary bladder, seminal vesicle, terminal part of ureter, vas deferens and prostate. Extensive anastomosis with branches of the SV could be recognized. No variations were observed in its origin, course and distribution in any of the male cadavers.
Uterine artery
The observations of the UA are based on 32 female pelvic halves. In all the cadavers it was tortuous and originated from the anterior division of the IIA and continued medially along the base of the broad ligament. It crossed the ureter at right angles and reached the cervix at the level of the internal os of the uterus. The UA then ascended along the lateral margin of the uterus within the broad ligament and ended by anastomosing with the ovarian artery. In addition, descending branches of the UA were observed along both sides of the supravaginal part of cervix that anastomosed with the ascending branches of the VA. No variations were observed in the origin, course and distribution of the UA.
Vaginal artery
The observations of the VA are also based on the same 32 female pelvic halves. In all the cadavers it originated from the anterior division of the IIA, and descended towards the vagina. The VA supplied branches to the anterior and posterior surfaces of the vagina, and adjacent parts of the urinary bladder and rectum. The individual branches of the VA could be seen anastomosing with descending branches of the UA. No anatomical variations were recognized in the origin, course and distribution of the VA.
Comparisons of the external diameters of uterine and vaginal arteries
Considering the variations in diameters of the UA and VA further analysis of all the female pelvic halves was carried out to determine if a relationship exists between the external diameters of these two arteries. In 21.88% pelvic halves, the external diameters of the UA were smaller than normal on both sides. Of these pelvic halves the VA was bilaterally large in 15.63% cadavers. In addition, of the 9.38% pelvic halves where the UA was bilaterally large, the VA was also bilaterally small in 6.25% pelvic halves.
DISCUSSION:
Mapping arterial variations and quantifying their dimensions is significant in both research and clinical settings, since they often serve as surrogates for determinates for vascular health. Heterogeneity in arterial dimensions represents a spectrum, the extremes of which represent pathological changes. The existing data in the literature on the IIA and its branches has focused on the origin, course, distribution and dimensions with very limited information on bilaterality, gender and racial variations. This underscores the need for reference databases to determine the efficiency of arterial circulation at a given anatomical point. Thus, the specific aim of this study was to compile normative data to add to the body of information regarding the origin, distribution and dimensions of the IIA and its branches.
Cadaveric derived information of specific arteries is fundamental to the interpretation of results of computerized angiographic studies. Methodological constraints can limit magnetic resonance angiography due to the limited resolution of smaller blood vessels within the pelvis, and the lack of bony landmarks. Conventional angiography of pelvic vessels have been reported to occasionally create a false impression of arterial occlusion within the pelvis because of slowing of blood flow through aberrant branches of the IIA. Similarly metal implants have also been reported to cause artefact formation in computerized tomography generated angiographic images. In addition, lower limb ischemia has at times been reported to be wrongly diagnosed because of erroneous placement of the catheter tip into aberrant branches of IIA. Lastly, since conventional Doppler is often limited in identifying deeply located arterial perforators, color Doppler is often usedm. However, the accuracy of color Doppler is dependent on human variations such as the experience of radiologist. Hence, a detailed cadaver-based identification is crucial in the management of bleeding in the pelvic cavity, avoidance of iatrogenic injury to the branches of IIA, treatment of uterine fibroids and the use of perforator flaps in reconstruction surgery.
All vascular dimensions in this study were recorded using electronic digital callipers which have been documented to have a high resolution and accuracy. In addition, the reliability of the methods of measurements used in this study have also been previously confirmed by three-dimensional digital image correlation (3D-DIC) studies, high resolution B-mode ultrasound and direct in vivo measurements. The accuracy of the measurements in this study were further reconfirmed by comparing dimensions obtained using slide calipers with measurements using digital stereo images of arteries using digital CCD Point Grey cameras with an image resolution of 1028×768 pixels (data not shown).
Since this study involved the analysis of dimensions of blood vessels of embalmed human cadavers, concerns can be raised about how reflective these values are of the actual living population. Such concerns are most relevant when cadavers have been rapidly frozen resulting in shrinkag, or rapidly filled with latex resulting in expansion of blood vessels. In this study, an appropriate volume of a modified Larssen solution was used for embalming which has been shown to prevent fragmentation of both soluble and non-soluble proteins, and ensuring adequate fixation of lipids and nucleic acids in cadavers. This ensures that the linear non-load-deformation characteristic of blood vessels is maintained in cadavers. In addition, the IIA and its branches containa high percentage of elastic tissue and smooth muscle in the tunica media, and hence are not prone to collapse. Therefore, concerns regarding the effect of distortion and shrinkage in cadavers that have been embalmed with a modified Larssen solution are largely unfounded.
A total of 30 male and 32 female pelvic halves were examined in this study. Variations were observed in the origin and branching patterns of the IIA and its branches, along with significant differences in the dimensions of some of the branches of the IIA.
CONCLUSIONS:
Due to the critical location of the IIA and its branches along the aorto-ilio-femoral arterial axis, and its collateral circulation, the IIA provides blood supply to the pelvic cavity, gluteal region and has the ability to develop a supplementary blood supply of the lower limbs. Hence a description of the IIA and its branches, will facilitate the acquisition of better clinical results, and avoid iatrogenic complications. Considering some of the limitations of computerized angiographic investigations, studies using embalmed human bodies are still vital in the elucidation of anatomical–morphological features. In addition, as diagnostic and interventional angiographic procedures become more popular, such information would be valuable in the prevention of interruption of circulation due to untargeted embolization of the surrounding organs.
REFERENCES:
Adachi B. (1928) Das Arteriensystem der Japaner. Kyoto: Maruzen 2, 136-142.
Ampatzidou F, Koutsogiannidis CP, Megalopoulos A, Trelopoulos G, Drossos G. (2019) Endovascular approach in chronic aortoiliac disease in patient undergoing coronary artery bypass surgery. Ann Card Anaesth 22, 96-97.
Arbatli H, Cikirikcioglu M, Pektok E, et al. (2010) Dynamic human cadaver model for testing the feasibility of new endovascular techniques and tools. Ann Vasc Surg 24,419-422.
Arfi A, Arfi-Rouche J, Barrau V, Nyangoh Timoh K, Touboul C. (2018) Three-dimensional computed tomography angiography reconstruction of the origin of the uterine artery and its clinical significance. Surg Radiol Anat 40, 85-90.
Athanaselis ED, Rountas C, Koutalos A, Dailiana Z, Malizos KN, Varitimidis SE. (2018) MR angiogram confirms sustained blood flow in 1, 2 ICSR artery of vascularized bone grafting in scaphoid nonunion treatment. Eur J Orthop Surg Traumatol 29, 343-348
Baldino G, Persi F, Mortola P, Gori A. (2018) An Alternative Technique to Achieve Haemostasis during PEVAR Using Perclose ProGlide. EJVES Short Rep 41, 8-9.
Bellier A, Chanet A, Belingheri P, Chaffanjon P.(2018) Techniques of cadaver perfusion for surgical training, a systematic review. Surg Radiol Anat 40,439-448.
Bilhim T, Pereira JA, Fernandes L, Rio Tinto H, Pisco JM. (2014) Angiographic anatomy of the male pelvic arteries. AJR Am J Roentgenol 203,W373-382.
Bonello VA, Bhangu A, Fitzgerald JE, Rasheed S, Tekkis P. (2014) Intraoperative bleeding and haemostasis during pelvic surgery for locally advanced or recurrent rectal cancer, a prospective evaluation. Tech Coloproctol 18,887-893.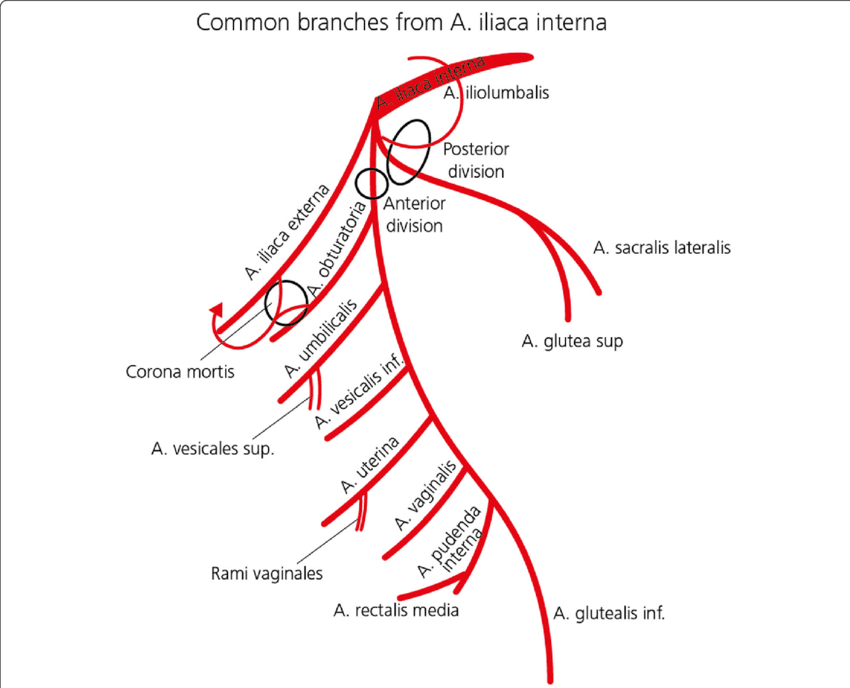
Articles from Amir Choudhary
View blog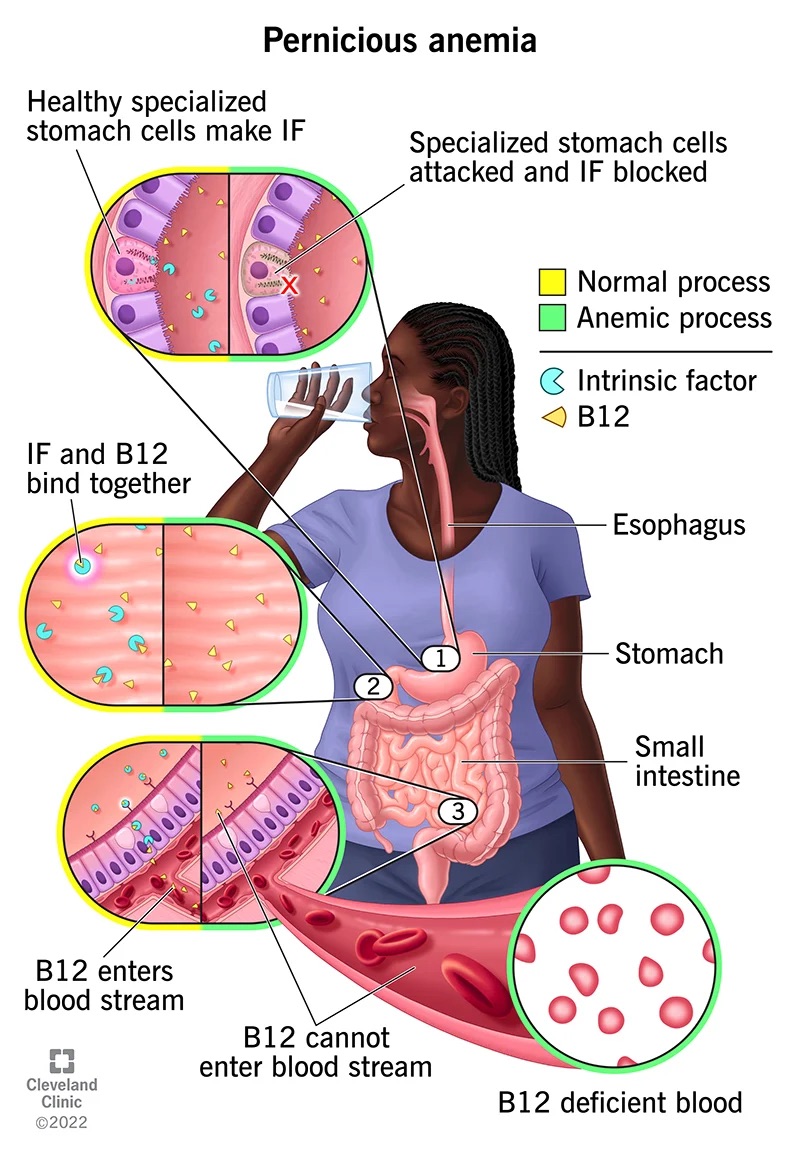
Abstract: Anemia is a blood disorder characterized by low levels of hemoglobin or red blood cells in ...

Abstract · Objective: This study aimed to analyze 100 most cited articles in breast cancer research. ...

STUDENT OF KARAGANDA MEDICAL COLLEGE (KMU), KARAGANDA, KAZAKHSTAN · CORRESPONDING AUTHOR; KHAN AMIR, ...
Related professionals
You may be interested in these jobs
-
Analysis Specialist
Found in: Talent IN C2 - 3 days ago
Nikkiso Clean Energy & Industrial Gases Vadodara, IndiaNikkiso Clean Energy & Industrial Gases is a leading provider of cryogenic pumps, fueling stations, heat exchangers, process systems, turboexpanders, services, and solutions for the liquefied natural gas (LNG), liquefied hydrogen (LH2), and industrial gases industries. We are a s ...
-

Manager - Marketing Compliance - BFSI (14-18 yrs)
Found in: beBee S2 IN - 3 days ago
iimjobs Hyderabad/Bangalore, India Full timeRoles & Responsibility: · - Manage a team responsible for establishing, implementing and maintaining risk standards and programs to drive compliance with federal, state, agency, legal and regulatory and Corporate Policy requirements · - Oversee the Front Line's execution and chal ...
-

Telecalling Internship
Found in: beBee S2 IN - 3 days ago
Fixitezy Delhi, India Internship, Full time· About the internship: · Selected intern's day-to-day responsibilities include convincing clients to visit our listed properties as per requirements. · > · Only those candidates can apply who: · 1. are available for full time (in-office) internship · 2. can start the internshi ...

Comments